Resolving Achilles Tendonitis
 The Achilles tendon is the strongest and largest tendon in the body. It is extremely vulnerable to injury due to its limited blood supply and the numerous forces to which it is subjected.
The Achilles tendon is the strongest and largest tendon in the body. It is extremely vulnerable to injury due to its limited blood supply and the numerous forces to which it is subjected.
The Achilles tendon is known as a co-joined tendon. This tendon directly joins into the Gastrocnemius and the Soleus muscle (calf muscles). The Achilles tendon transmits the force of the calf muscles (Gastrocnemius and Soleus) to produce the push-off during walking, running, and jumping.
The area of the tendon (approximately 2 to 6 cm above its insertion into the Calcaneus) has the poorest blood supply, and therefore heals the most slowly. This makes it extremely susceptible to injury.
Click on the following tabs for more information about the types and causes of Achillles Tendonitis.
Common Injuries to the Achilles Tendon
 Athletes suffer from three common types of injury to the Achilles Tendon:
Athletes suffer from three common types of injury to the Achilles Tendon:
- Paratenonitis – usually referred to as Achilles Tendonitis.
- Tendinosis. – This is usually a non tender palpable nodule or cord at the Achilles tendon.
- Rupture of the Tendon (either partial or complete).
Paratenonitis:
- Is an inflammation of the Paratenon – a sheath surrounding the Achilles tendon. Paratenonitis is often caused by repetitive strain or over-use. This injury is common in triathletes.
Tendinosis:
- Refers to degeneration within the tendon due to a previous tear.
- This condition can be felt as a palpable tendon nodule very close to the heel. The nodule is formed by the accumulation of scar tissue.
- Circulation to the Achilles tendon is very poor, especially near the heel, resulting in poor oxygen supply. This results in poor healing and formation of microscopic tears, causing the tendon to thicken.
- Chronic Achilles Tendinosis can lead to a complete rupture if it is not treated and rehabilitated correctly. If not addressed, this condition may be a warning sign of worse things to come.
Ruptured Tendon:
- A complete rupture is where the tendon has completely separated from the Calcaneus (heel bone). This can occur when Paratenonitis and Tendinosis were not correctly treated and rehabilitated.
- Surgical intervention is the only solution to this condition.
Consider the Kinetic Chain Structures
Any restrictions in the kinetic chain of the Achilles tendon, either above or below the tendon, can affect the functioning of the Achilles tendon. Such structures would include:
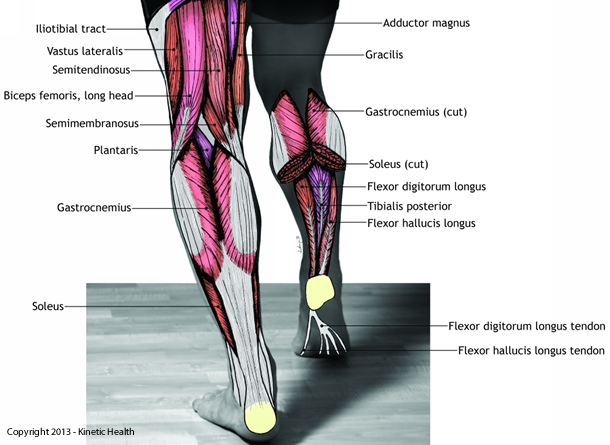
- Hamstring muscles – The upper portion of the Gastrocnemius (superficial calf muscles) are in contact with Biceps Femoris, Semitendinosus, and Semimembranosis (three sections of the hamstrings).
- Plantaris muscle – This muscle inserts into the middle one third of the posterior calcaneal surface (heel bone), just on the inside of the Achilles Tendon.
- Popliteus muscle – This muscle is involved in medial knee rotation. When it is restricted, it may cause increased stress on the lower extremities.
- Flexor Hallicus Longus, Flexor Hallicus Brevis, and the Tibialis Anterior muscles. These muscles are involved in cases of increased pronation and hyperpronation.
The illustration below shows the posterior muscles that are located further up the kinetic chain from the Achilles Tendon.
Resolving Achilles Tendonitis
Effective Treatments for Achilles Tendonitis should be preceded by careful diagnosis and identification of affected structures, and then appropriate soft-tissue treatments with techniques such as Active Release, and customized exercise routines that address all the affected kinetic chain elements. Click on the each of the following tabs for more details about this process.
Using ART to Treat Achilles Tendonitis
Active Release Techniques (ART®) is very successful at treating this type of injury since it removes restrictive adhesions between  both the superficial and deep tissue structures along the entire kinetic chain.
both the superficial and deep tissue structures along the entire kinetic chain.
Trained ART practitioners perform a biomechanical analysis of athletes to determine where the restrictions are located along the entire kinetic chain. ART treatments are specific and based upon the individual needs of each athlete. It is not a cookbook approach to treating a non-specific diagnosis.
For example:
- If the fascial tissue anterior to the tendon is restricted (which commonly occurs in this condition), ART procedures can be used to release the adhesions.
- Other structures in the kinetic chain are similarly treated.
ART® finds the specific tissues that are restricted and physically works them back to its normal texture, tension, and length by using various hand positions and soft tissue manipulation methods. While breaking up the adhesions can be uncomfortable at times, it is important to reproduce the symptoms.
Effective treatment of the Achilles tendon, or of any soft tissue injury, requires an alteration in tissue structure that breaks up the restrictive cross-fiber adhesions and restores normal function to the affected soft tissue areas. When executed properly, this process substantially decreases healing time, treats the root cause of the injury, and improves athletic performance.
With ART we often see immediate improvement after treating the involved structures.
More Information about Achilles Tendonitis
Dr. Abelson provides a broad range of information to his patients and the public. They range from published books (eBook and hard-copy), to blogs, YouTube Videos, websites, and articles. Click on the following tabs to access some of his more popular information resources.
Books for Resolving Achilles Tendonitis
Release Your Pain: 2nd Edition
Dr.Abelson’s international best-seller – Release Your Pain – provides a detailed description about the anatomy, kinetic chain, and causes of Achilles Tendonitis. It discusses means for resolving this condition, and provides specially selected exercises to help you begin the process of resolution. Visit our website at www.releaseyourbody.com to purchase your eBook or hard-Copy.
Blogs about Achilles Tendonitis
Click on the following blog articles for additional information on Achilles Tendonitis.
 Achilles Tendonitis or Tendinopathy
Achilles Tendonitis or Tendinopathy
The Achilles Tendon is the strongest and largest tendon in the body. It is extremely vulnerable to injury due to its limited blood supply and the numerous forces to which it is subjected. The Achilles Tendon is known as a co-joined tendon. This tendon joins directly into the calf muscles (gastrocnemius and soleus).
For more information about our clinic in Calgary, Alberta, please visit www.kinetichealth.ca.